 Randomized Clinical Trial for Treatment of Atrioventricular Nodal Reentry Tachycardia (AVNRT): Low Voltage and Propagation Mapping vs. Anatomic/Electrogram Approach to Slow AV Nodal Pathway Ablation
Randomized Clinical Trial for Treatment of Atrioventricular Nodal Reentry Tachycardia (AVNRT): Low Voltage and Propagation Mapping vs. Anatomic/Electrogram Approach to Slow AV Nodal Pathway Ablation
Significance:
AVNRT is the most common arrhythmia in adults until the onset of Atrial Fibrillation. Though this arrhythmia is commonly treated by ablation, complications and recurrences continue to occur. If we can demonstrate that voltage and propagation wave mapping requires less ablation sites, decreases procedure time, and results in a decreased risk of complication/recurrence, this 3D mapping radiation free technique may become the gold standard approach for ablation of this arrhythmia.
Background:
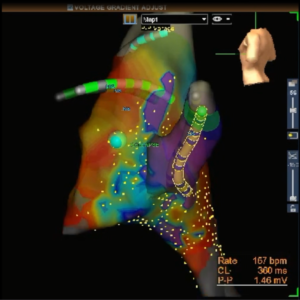
While a conceptual construct for understanding AVNRT has evolved over the years, the subtleties of the pathophysiologic mechanism leading to its occurrence is undefined. Approaches for ablation of the slow AV nodal pathway differ among pediatric centers. Two commonly used techniques involve: 1) an anatomical/electrogram approach based on physical position of the ablation catheter and the electrogram morphology (Anatomical/electrogram Technique), and the more recent 2) voltage and propagation mapping to ablate over a site of low voltage and late activation in the triangle of Koch, as often seen at a site of a propagation wave collision. (Voltage/Propagation technique).
Though recent studies have suggested that voltage and propagation mapping can provide an accurate radiation free technique for localization of the slow pathway, the studies are retrospective and not compared to the more typical anatomical/electrogram based technique. We propose a prospective comparative study of the effectiveness and safety of these two techniques for modification of slow AV nodal pathway.
Specific Aim:
Define and compare the effectiveness and safety of two technical approaches to the ablation of slow AV nodal pathway conduction in the treatment of AVNRT.
Hypothesis:
The effectiveness and safety of modifying slow AV nodal pathway conduction underlying AVNRT can be improved using voltage and propagation mapping to identify an area of low voltage and late activation, often at a site of propagation wave collision. This voltage/propagation mapping ablation technique compared will be compared to the current anatomical/electrogram ablation technique. The number of ablations necessary to achieve successful modification of slow AV nodal pathway conduction will be our primary end point. Secondary end points will include: the length of time needed to modify slow AV nodal pathway conduction, the recurrence rate of AVNRT, and the incidence of acute injury to the AV node that occurs during the ablation procedure will be compared.
Methods:
Targeted Enrolment: 300 patients with AVNRT
Targeted Total Centers: 10 or more centers
Pediatric centers included, age <22 years.
Leading Centers:
Dr. Nicholas Von Bergen,
University of Wisconsin, Madison, WI
Director of Electrophysiology Laboratory, Madison, WI
vonbergen@wisc.edu
Dr. Ian Law,
University of Iowa, Iowa City, IA
Director, Pediatric Cardiology
ian-law@uiowa.edu
Dr. Jeff Moak,
Children’s National, Washington DC
Director, Electrophysiology and Pacing
JMOAK@childrensnational.org